Taking a biopsy from the edge of a skin lesion becomes a less traumatic procedure if the sliver to be removed is first transfixed by a fine silk stitch.
The biopsy of skin lesions such as suspected cancers can be untidy and damaging, with much bleeding and an unnecessarily large defect. This is particularly upsetting on the face of a patient. The usual biopsy technique seems to be to Cut a wedge of tissue from the edge of a lesion while trying to grip it in a pair of toothed dissecting forceps. It is difficult to control the length and depth of the cut, and it is especially hard to grasp just a small sliver of tissue with the dissecting forceps. Among dermatologists it is common practice to use a special cylindrical punch, which is rotated to cut out a small disc of tissue but does not yield the desirable shape of a segment of a pie.
A simple technique which has seemed satisfactory to the writer is to transfix the edge of the lesion with a fine atraumatic radially-placed suture of 5/0 or 6/0 silk. First the patient's skin is prepared with the usual antiseptic. Then it is draped with a single sterile paper towel, from which a central two or three centimetre circle has been removed by folding the paper twice and cutting off the corner. (Wetting the paper with a little antiseptic helps it to stick on to the skin, if it is not too irregular, and so prevents a little dribble of blood causing a mess.) Then, rather less than half a millilitre of local anaesthetic is injected very slowly just under the proposed biopsy site.
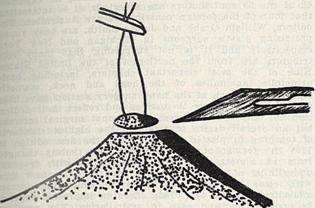 Fig 1.The transfixing suture described is inserted very deliberately as a bite about three millimetres long and a millimetre deep.
Fig 1.The transfixing suture described is inserted very deliberately as a bite about three millimetres long and a millimetre deep.
With two ends of the suture held a couple of centimetres long in a pair of mosquito forceps, a little traction will tent up the tissues so that a little wedge can be cut away with two careful strokes of the point of a number 11 blade (Figure 1).
A dry dressing is then held steadily on to the excision site, and replaced after a few minutes with a Band-aid. Meanwhile, the sliver of tissue, together with its transfixing suture, is placed in formol-saline or some other preservative in a labelled specimen. bottle in the usual way. Often it takes a special effort to remember to submit some unfixed tissue in a sterile container for bacteriological examination.
The technique of transfixing small lesions, for biopsy or in their entirety, is not used nearly often enough. The best toothed dissecting forceps are not adequate to grip many surface lesions, and one rarely has the best quality. A common repeated sequence of movements (" therbligs ") in this situation is " gripslip-oops ". If the stay suture has been passed through unhealthy tissue the same thread should not be used for later suturing of any skin defect.
Michael Patkin 20 Brimage Street, Whyalla, S.A. 5600.
Address for reprints: Mr M. Patkin, Brimage House, 20 Brimage Street, Whyalla, S.A. 5600.
-o0o-